So I’ve had a couple of people (therapists) ask how such results were achieved with the shoulder yesterday.
First we examined the dynamics of the fall, including a pretty picture (client drawn 😉) of impact sites, and angles of arms / rotations etc.
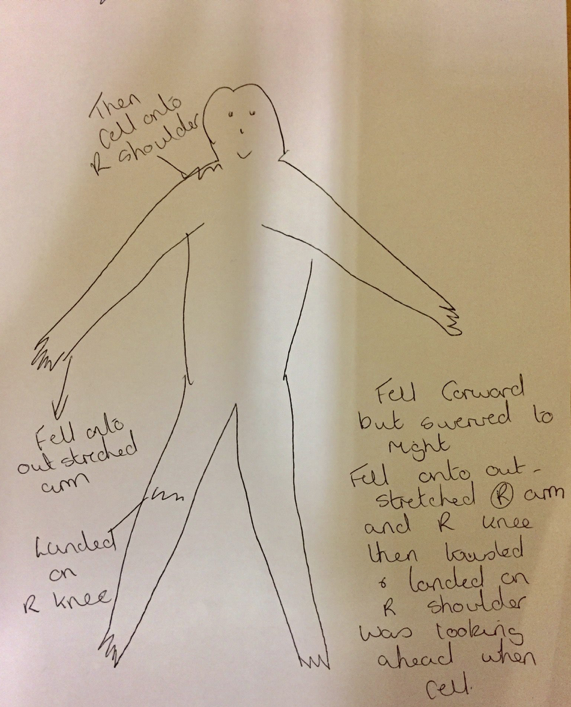
Client image
From this it seemed likely there would have been some eye dysfunction present. We checked this with the standard protocol. The results were unclear as to which pattern was involved as a number of patterns revealed nystagmus.
We moved on to testing the extra ocular muscles, and found a few dysfunctional. We linked the pair to GA’s and bingo 😊👍🏻
Once resolved and more of the arm muscles working, we moved onto the standard GH De/Compression testing, resolved that, and revideoed.
Job done.
Pairs in initial dysfunction: R Tricep, Subscap, Lat, LTrap, PecMn, LevScap, PubiTubi, IngLig, Iliac crest, L longus colli, L Subscap, L GMx.
Compression linked to posterior capsule and bicep.
I adapt the level 3 protocol to identify all muscles which pair with a higher level dysfunction, and then to prioritise them (which wasn’t taught on the course I attended, just something I’ve discovered with trial and error). It makes setting HW super easy and effective 👍🏻
Happy to discuss this via PM if you’re a level 3 but obviously intellectual property rights for NKT preclude me from doing this for anyone else 🤷🏻♂️
Hope this helps 🤩
Experience the difference – A refreshingly different approach to pain and dysfunction, so you can breathe better, move better, to live better.